

Overview
Traumatic Brain Injury (TBI) is sudden damage to the brain caused by a blow or jolt to the head. Common causes include car or motorcycle crashes, falls, sports injuries, and assaults. Injuries can range from mild concussions to severe permanent brain damage. While treatment for mild (traumatic brain injury) TBI may include rest and medication, severe TBI may require intensive care and life-saving surgery. Those who survive a brain injury can face lasting effects in their physical and mental abilities as well as emotions and personality. Most people who suffer moderate to severe (traumatic brain injury) TBI will need rehabilitation to recover and relearn skills.
What is a traumatic brain injury?
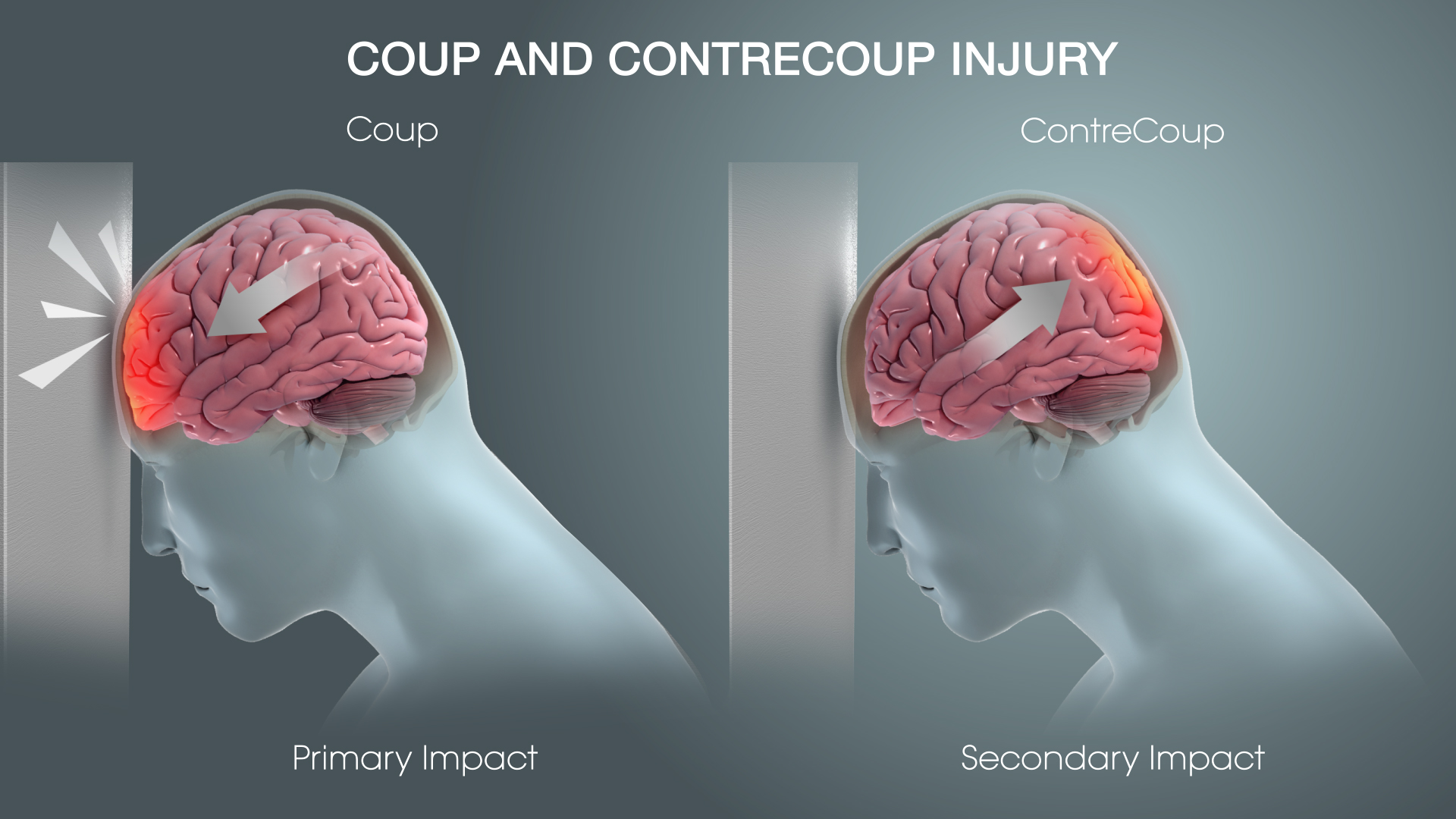
TBI (traumatic brain injury) is an injury to the brain caused by a blow or jolt to the head from blunt or penetrating trauma. The injury that occurs at the moment of impact is known as the primary injury. Primary injuries can involve a specific lobe of the brain or can involve the entire brain. Sometimes the skull may be fractured, but not always. During the impact of an accident, the brain crashes back and forth inside the skull causing bruising, bleeding, and tearing of nerve fibers. Immediately after the accident the person may be confused, not remember what happened, have blurry vision and dizziness, or lose consciousness. At first the person may appear fine, but their condition can decline rapidly. After the initial impact occurs, the brain undergoes a delayed trauma (it swells) pushing itself against the skull and reducing the flow of oxygen-rich blood. This is called secondary injury, which is often more damaging than the primary injury.
Symptoms
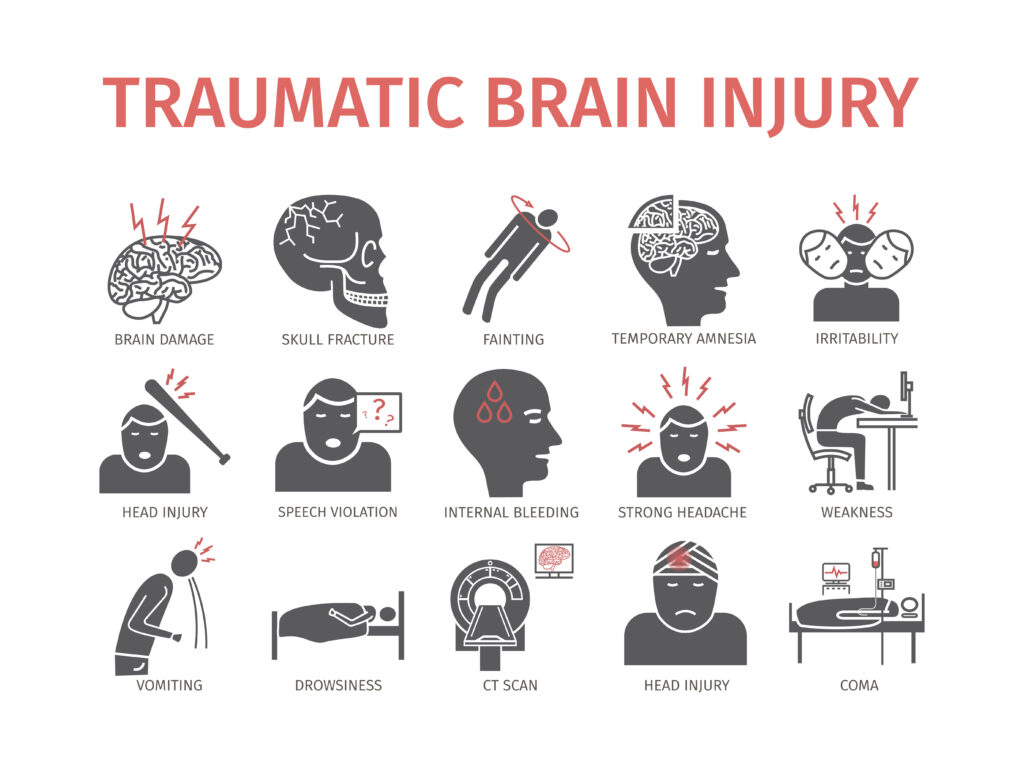
Symptoms vary greatly depending on the severity of the head injury. They may include any of the following:
- Vomiting
- Lethargy
- Headache
- Confusion
- Paralysis
- Coma
- Loss of consciousness
- Dilated pupils
- Vision changes (blurred vision or seeing double, unable to tolerate bright light, loss of eye movement, blindness)
- Cerebrospinal fluid (CSF) (clear or blood-tinged) appear from the ears or nose
- Dizziness and balance concerns
- Breathing problems
- Slow pulse
- Slow breathing ratewith an increase in blood pressure
- Ringing in the ears or changes in hearing
- Cognitive difficulties
- Inappropriate emotional responses
- Speech difficulties (slurred speech, inability to understand and/or articulate words)
- Difficulty swallowing
- Body numbness or tingling
- Droopy eyelid or facial weakness
- Loss of bowel control or bladder control
Types of traumatic brain injuries
TBIs (traumatic brain injury) can cause “mass lesions,” w an area of localized injury such as hematomas and contusions that increase pressure within the brain. Summarized below are different types of sequelae deveoped from (traumatic brain injury) TBIs:
Hematoma:
A hematoma is a blood clot within the brain or on its surface. Hematomas may occur anywhere within the brain. An epidural hematoma is a collection of blood between the dura mater (the protective covering of the brain) and the inside of the skull. A subdural hematoma is a collection of blood between the dura mater and the arachnoid layer, which sits directly on the surface of the brain.
Contusion:
A cerebral contusion is bruising of brain tissue. When examined under a microscope, cerebral contusions are comparable to bruises in other parts of the body. They consist of areas of injured or swollen brain mixed with blood that has leaked from arteries, veins, or capillaries. Most commonly, contusions are at the base of the front parts of the brain, but may occur anywhere.
Intracerebral Hemorrhage:
An intracerebral hemorrhage (ICH) describes bleeding within the brain tissue, may be related to other brain injuries, especially contusions. The size and location of the hemorrhage helps determine whether it can be removed surgically.
Subarachnoid Hemorrhage:
Subarachnoid hemorrhage (SAH) is caused by bleeding into the subarachnoid space. It appears as diffuse blood spread thinly over the surface of the brain and commonly after TBI. Most cases of SAH associated with head trauma are mild. Hydrocephalus may result from severe traumatic SAH.
Diffuse Injuries:
TBIs can produce microscopic changes that do not appear on CT scans and are scattered throughout the brain. This category of injuries, called diffuse brain injury, may occur with or without an associated mass lesion.
Diffuse Axonal Injury:
Axonal injury refers to impaired function and gradual loss of axons.These long extensions of nerve cells enable them to communicate with each other. If enough axons are harmed in this way, the ability of nerve cells to communicate with each other and to integrate their function may be lost or greatly impaired, possibly leaving a patient with severe disabilities.
Ischemia:
Another type of diffuse injury is ischemia or insufficient blood supply to certain parts of the brain. A decrease in blood supply to very low levels may occur commonly in a significant number of TBI patients. This is crucial since a brain that has just undergone a traumatic injury is especially sensitive to slight reductions in blood flow. Changes in blood pressure during the first few days after head injury can also have an adverse effect.
Skull Fractures: Linear skull fractures or simple breaks or “cracks” in the skull may accompany (traumatic brain injury) TBIs.
Possible forces, strong enough to cause a skull fracture may damage the underlying brain. Skull fractures may be alarming, if found on a patient evaluation. Fractures at the base of the skull are problematic since they can cause injury to nerves, arteries, or other structures. If the fracture extends into the sinuses, a leakage of cerebrospinal fluid (CSF) from the nose or ears may occur. Depressed skull fractures, in which part of the bone presses on or into the brain, can also occur.
Testing and Diagnosis

Anyone with signs of moderate or severe (traumatic brain injury) TBI should receive medical attention as soon as possible. Because we cannot do much to reverse the initial brain damage caused by trauma, medical providers try to stabilize an individual with (traumatic brain injury) TBI and focus on preventing further injury.
First, the cardiac and pulmonary function is assessed. Next, a quick examination of the entire body is performed, followed by a complete neurological examination. The neurological examination includes an assessment utilizing the Glasgow Coma Scale (GCS). In addition to the GCS, also tested is the ability of the pupils to become smaller in bright light. In patients with large mass lesions or with high intracranial pressure (ICP), one or both pupils may be very wide or “blown.” The presence of a wide or dilated pupil on only one side suggests a large mass lesion may be present. Brainstem reflexes including gag and corneal (blink) may also be tested.
Radiological Tests
A computed tomography scan (CT or CAT scan) is the gold standard for the radiological assessment of a (traumatic brain injury) TBI patient. A CT scan is easy to perform and an excellent test for detecting the presence of blood and fractures, the most crucial lesions to identify in medical trauma cases. Plain x-rays of the skull are recommended by some as a way to evaluate patients with only mild neurological dysfunction. However, most centers in the U.S. have readily available CT scanning, a more accurate test, rendering the routine use of skull x-rays for (traumatic brain injury) TBI patients to decline.
Magnetic resonance imaging (MRI) is not commonly used for acute head injury since it takes longer to perform a MRI than a CT. Because it is difficult to transport an acutely-injured patient from the emergency room to a MRI scanner, the use of MRI is impractical. However, once a patient is stabilized, MRI may demonstrate the existence of lesions that were not detected on the CT scan. This information is generally more useful for determining prognosis than for influencing treatment.
Treatment

Surgery
Many patients with moderate or severe head injuries head directly from the emergency room to the operating room. In many cases, surgery is performed to remove a large hematoma or contusion that is significantly compressing the brain or raising the pressure within the skull. After surgery, these patients are under observation in the intensive care unit (ICU).
Other head-injured patients may not head to the operating room immediately, instead are taken from the emergency room to the ICU. Since contusions or hematomas may enlarge over the first hours or days after head injury, immediate surgery is not recommended on these patients until several days after their injury. Delayed hematomas may be discovered when a patient’s neurological exam worsens or when their ICP increases. On other occasions, a routine follow-up CT scanto determine whether a small lesion has changed in size indicates that the hematoma or contusion has enlarged significantly. In these cases, the safest approach is to remove the lesion before it enlarges and causes neurological damage.
During surgery, the hair over the affected part of the head is usually shaved. After the scalp incision, the removed bone is extracted in a single piece or flap, then replaced after surgery unless contaminated. The dura mater is carefully cut to reveal the underlying brain. After any hematoma or contusion is removed, the neurosurgeon ensures the area is not bleeding. He or she then closes the dura, replaces the bone and closes the scalp. If the brain is very swollen, some neurosurgeons may decide not to replace the bone until the swelling decreases, which may take up to several weeks. The neurosurgeon may elect to place an ICP monitor or other types of monitors if these were not already in place. The patient is returned to the ICU for observation and additional care.
Non-Surgical Treatments
At present, medication administered to prevent nerve damage or promote nerve healing after TBI not available. The primary goal in the ICU is to prevent any secondary injury to the brain. The “primary insult” refers to the initial trauma to the brain, whereas the “secondary insult” is any subsequent development that may contribute to neurological injury. For example, an injured brain is especially sensitive and vulnerable to decreases in blood pressure otherwise well tolerated. One way to avoid secondary insults is to attempt normal or slightly elevated blood pressure levels. Likewise, increases in ICP, decreases in blood oxygenation, increases in body temperature, increases in blood glucose and many other disturbances can potentially worsen neurological damage. The major role of ICU management is the prevention of secondary insults in head-injured patients.
Various monitoring devices may assist health care personnel in caring for the patient. Placement of an ICP monitor into the brain can help detect excessive swelling. One commonly used type of ICP monitor is a ventriculostomy, a narrow, flexible, hollow catheter that is passed into the ventricles, or fluid spaces in the center of the brain, to monitor ICP and drain CSF if ICP increases. Another commonly used type of intracranial pressure monitoring device involves placement of a small fiberoptic catheter directly into the brain tissue. Additional catheters may be added to measure brain temperature and brain tissue oxygenation. Placement of an oxygen sensor into the jugular vein can detect how much oxygen the brain is using. This may be related to the degree of brain damage. Many other monitoring techniques currently under investigation to determine whether they can help improve outcome after head injury or provide additional information about caring for (traumatic brain injury) TBI patients.